

Friday, August 5 at 5:00 pm. For those of you in the military, that is 1700 hrs. That is your last chance to submit comments on the Proposed rule for Home Health for FY 2023. If your opinion coincides with mine, well, that’s just great. If it doesn’t, you should still submit your opinion. CMS needs to know we are interested in what is happening in our industry.
There is a lot written in the regulations. Much of it doesn’t pertain to nursing but a long justifications for the new rule is explained in tedious detail within the regulations
which won’t appeal to field nurses and case managers with a full schedule. As best as I can, I will try to summarize the information that I think is important to nurses.
Assumptions about Agencies (You)
Medicare assumes that PDGM will affect the way that we assess and document patient care. Here are the three assumptions discussed in the regs.
- Agencies will upcode
- Agencies will add unnecessary visits to avoid LUPAs
- Agencies will add erroneous diagnoses to improve comorbidities.
Psychiatric Nursing
Revised PDGM Scoring will result in a 1.3 Billion dollar reduction in payment for psychiatric nursing. This is in the light of multiple studies noting the negative effects of the pandemic and now, the economy on mental health. The Olmstead ruling from the Supreme Court in 1999 states that patients must be treated in the least restrictive environment. Without psych nurses to administer and monitor the effects of psych meds, are we forcing more of our elderly into unwanted institutionalism? To be clear, both mental health and payment for services are declining at the same time. This does not bode well. Taken off the spreadsheet and placed in agencies, it means that patients who require a lot of care will be admitted to hospitals because home health will not be able to afford taking care of them.
Covid Effects
This is directly from the misguided regulations:
For CY 2023 rate setting, we do not anticipate significant differences between using pre COVID-19 PHE data (CY 2019 claims) and the most recent claims data at the time of rulemaking (CY 2021 claims). Look at the clinical groupings before the start of the pandemic and for the first two years. The data for 2018 and 2019 was simulated because of the change to 30 day claim periods.
Here is the data they use to support that delusion. Look at differences between 2019 and 2020 and note that they are sustained throughout 2021.

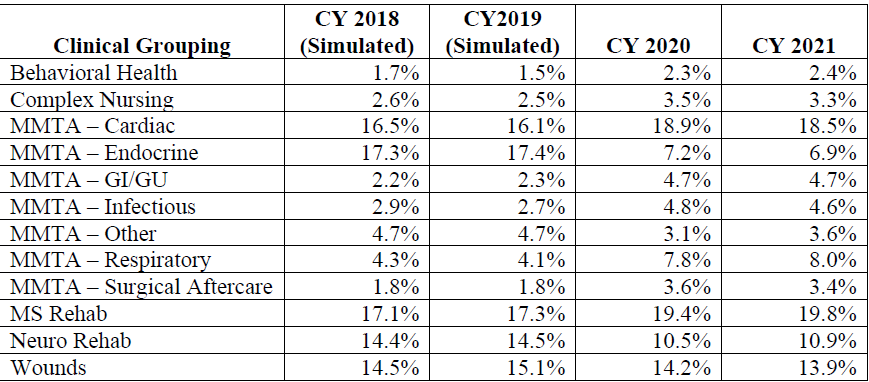
In 2020 the percentage of patients who fell into the behavioral health grouping jumped from 1.5 to 2.3. Cardiac groupings went up slightly while endocrine fell appreciably. Could this be because it was diluted by respiratory? Between 2019 and 2021 the number of admissions with a respiratory grouping doubled. During this period of time, there were no diagnosis codes for Long Covid or any after effects. Surgical aftercare also doubled. Could this be because elective surgeries were canceled and the remaining patients were of higher acuity and more prone to infections and slower healing? Are these changes really insignificant or is that a way of ignoring them so the price decreases can be justified?
Telemedicine
Although there is no mention of additional payment or telemedicine substituting for actual visits, Medicare proposes to collect data on home health telemedicine. I strongly suggest you do this regardless. Be aware that the DOJ just arrested some folks who, collectively are charged with 1.2 Billion in telemedicine fraud. If ever it is a billable skill, it might be an idea to do it right. Telemedicine could enhance our delivery of care or present a new opportunity to be charged for fraud.
Health Disparities
Having read the headlines, CMS is aware that there are significant disparities in care rendered to Black and Hispanic patients. I strongly support the interest taken in health disparities but at this point, no mandated changes have been levied on home care agencies. There are some suggestions, though and in the interest of quality patient care across the board, I suggest that agencies begin thinking about the answers to these questions posed in the proposed regs:
- What efforts does your HHA employ to recruit staff, volunteers, and board members from diverse populations to represent and serve underserved populations? How does your HHA attempt to bridge any cultural gaps between your personnel and beneficiaries/clients?
- How does your HHA measure whether this has an impact on health equity?
- How does your HHA currently identify barriers to access to care in your community or service area?
- What are the barriers to collecting data related to disparities, SDOH, and equity? What steps does your HHA take to address these barriers?
- How does your HHA collect self-reported demographic information such as information on race and ethnicity, disability, sexual orientation, gender identity, veteran status, socioeconomic status, and language preference?
- How is your HHA using collected information such as housing, food security, access to interpreter services, caregiving status, and marital status to inform its health equity initiatives?
I think a better term than health disparities and inequities would be care inequity or disparity. When an 87 yo Black Male with hypertension is admitted to an agency after years of being treated (or not treated) in an environment of health disparities, you are not going to erase the damage done in a single episode but he deserves the very best care you can give. That might mean going out of your comfort zone or spending extra time finding suitable food, meds, conferring with Social Workers and other providers but it is worth it. Just ask the patient.
Medicare has proposed variances in scoring in the Black and Hispanic communities and./or measurement of social determinants of health (SDOH) to capture the disparities in care with the eventual goal of adopting a reportable measure. More importantly, they have asked for your comments. My biggest complaint is usually that nobody asked us for our opinion. This time they are and I suggest that you take advantage of it. I know I will.
Please read the regulations in their entirety and form your own opinions. And then comment. We do have a voice. Let’s use it.