The Scapegoat

I have spent the morning reading and re-reading the complaint survey related to the death of a patient who gave Vecuronium instead of Versed at Vanderbilt University hospital. Clearly the nurse made a costly mistake. She was prosecuted and convicted of two felonies.
The complaint survey was conducted almost a year after the death. Vanderbilt Hospital did not report the death so there was no reason for the surveyors to conduct a complaint survey. The death is rumored to be reported by an anonymous tip. The irresponsibility demonstrated by Vanderbilt university in not reporting a patient death due to a medication error is a clear violation of minimum standards but don’t worry. They have changed their policy.
This tragic death occurred when the patient was sent for a PET scan. It is noted that the patient was received in radiology awake and alert but anxious. That’s when the Versed was ordered. Why pray tell, did the response to the state survey focus so intensely on the transport policy.
Radanda Vaught gave what she believed to be Versed. The radioactive dye had already been given and the patient was placed in a room while the dye dispersed throughout her system.
The radiology techs acknowledged that video monitoring was in place but the cameras could not discern the movement of breathing in a patient. Not wanting to sound callous, a patient who dies from Versed looks about the same as one who died from Vecuronium. I can afford a Ring Doorbell and it would let me know if someone was breathing. Can Vanderbilt University Hospital not afford a trip to Best Buy? Even if they shelled out the cash for quality equipment, the best camera in the world is not a Registered Nurse.
Something that was completely glossed over in all the chatter is the surveyor’s account of the interview with the radiology tech. Please read carefully. I have chosen to not summarize in case I am wrongly interpreting this.
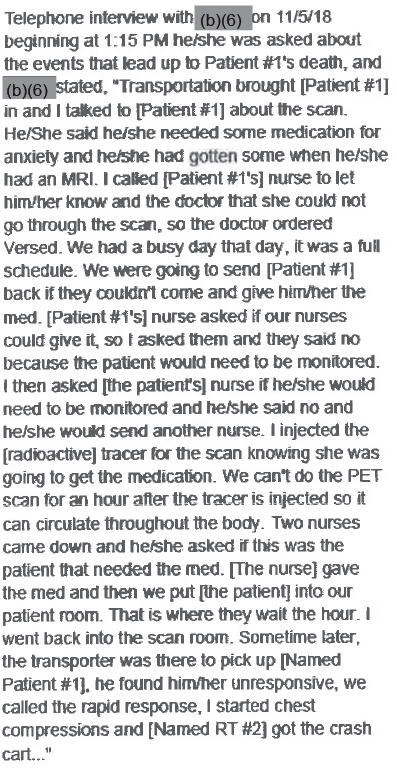
Because surveys are public information, names are substituted and frankly it can be confusing. My assumption is the nurse who was referred to as the patient’s nurse was the one assigned the patient that morning and the nurses sent were the resource nurse (Vaught) and her preceptee. Please read and let me know if you interpret it differently because it appears as though an ICU nurse told radiology that the patient did not require monitoring after the administration of Versed.
I don’t make this stuff up. This is extracted from the Versed package insert in one of those ominous black boxes.
Intravenous midazolam should be used only in hospital or ambulatory care settings, including physicians’ and dental offices, that provide for continuous monitoring of respiratory and cardiac function, e.g, pulse oximetry. Immediate availability of resuscitative drugs and age- and size-appropriate equipment for bag/valve/mask ventilation and intubation, and personnel trained in their use and skilled in airway management should be assured.
So I have questions. If the patient had her pulse oximetry monitored or a portable ekg, would an alarm have alerted staff to a problem before a transport tech happened to walk by and notice the patient was not breathing? Monitors do not take the place of a nurse but they are better than nothing.
So, the fact that the wrong drug was given probably didn’t affect the outcome because if Versed was given according to evidence based practice standards, monitoring would have been in place and lots of alarms would have sounded and there would have been an ambu bag and someone qualified to intubate right there.
Back to the transport policy which has been revised to include critical care patients. As of November 27, 2018 all patients will be ‘transferred with the equipment and supplies, and staff appropriate to monitor and support the patient’s physiological needs’. What on earth did the policy say before it was revised.
The Transport Policy also includes provisions that after arrival at the receiving department/unit, if a patient requires continuous monitoring, a clinical staff member is required to be available to receive handover of the patient pursuant to the Hospital’s CL SOP – Clinical Handover Communication. Who might this clinical staff member be? I would hope a Registered Nurse experienced in conscious sedation would be the least qualified person allowed, assuming anesthesia wasn’t available.
Remember, the radiology department refused to give the Versed because no nurse was available to monitor the patient. This change in policy doesn’t appear useful.
The argument against Ms. Vaught is that she fell short of accepted nursing standards. There is no doubt in my mind. There is also no doubt in my mind that Radonda Vaught, given the chance to practice again, will never make this or a similar mistake again.
Vanderbilt University Medical Center, on the other hand, will continue to suffer the very bad outcomes of disinterested leadership concerned with image rather than patient care unless something has changed or will change.
Don’t let this discourage you from reporting errors. Ms. Vaught’s patient is not the only one who died from a med error. Every day, med errors harm patients. Home Health and hospice are not exceptions. Let this be a reminder to reconcile your meds, be mindful and learn from your mistakes before they result in the death of a patient.



This whole thing is terrifying. The lackadaisical atmosphere of the situation is appalling. It’s OK to put a patient who’s had a brain bleed in a room, alone, without anyone there watching her for an hour? NO. That’s ridiculous. She could have had a reaction to the dye that was injected. How do we know she didn’t? I only gave Versed once and that was when I was a House Supervisor. It was a kid with a broken arm in ER. He had on a monitor with O2 sat and I stayed with him till he woke up after the arm was set and casted. The doctor only left the room briefly to get something, but he was right there if I needed him. I can’t imagine her (Vaught) just leaving a patient there after giving what she thought was Versed, or any sedative for that matter. The patient’s nurse said that no, the patient would not need to be monitored after the Versed? What? Ms. Vaught did indeed fall short of her nursing standards. Several people fell short of their standards from what I’ve read in this and other versions. The hospital fell short of every ethical and medical standard I can think of and all they are going to do is give the family money and instruct them not to talk about it. I am so conflicted though about her “guilt” or “innocence.” She isn’t “innocent” but is she a criminal? She may go to prison with murderers, prostitutes, thieves, and all sorts of unsavory people. What could that possibly achieve? What could happen to her in there? Who will she be when she gets out? I am so glad I’m retired.
I will tell you what it won’t achieve – improved patient safety. If I had made the same error no amount of jail time could make me feel worse.
I have spent the last 2 hours reading about this case. I know there was a medication error that caused the death of a human being.
However, I am asking myself again and again why this hospital is not accountable for this as well? Clearly, there were errors from their part as well.
I wish Ms Vaught well, and hope nurses do not get discouraged.
My fear is that nobody will report errors. I can hardly condone a fatal med error but does she belong in jail? Let he without sin cast the first stone.
Horrifying, yet we all know the variables that are present in every setting that lead to these kinds of errors. I do not believe the charges were justified, though she clearly was negligent. Who would go into nursing knowing that mistakes will not just cost you your livelihood and your license, but they might buy you prison time? You cannot be human. You must be perfect, always, against impossible odds. The main thing they need to do is to make a two nurse check for overrides. She overrode the system to pull the wrong med. She ignored warning labels- desensitized no doubt from working with high risk meds all the time. But if two nurses had checked- the odds are that the extra mental work that it requires would have forced them to read that label and notice it was the wrong drug.
It may be there but I didn’t see much about her HR records. Was she qualified. Signed off?
Someone at Vanderbilt knew better than to give Versed without monitoring. And why was Vec in an ADC? Maybe instead of an exception, paralytics, concentrated K+, and other meds with very low safety levels should require reentry of credentials – something that doesn’t significantly delay care but the very presence of that requirement notifies the nurse that they are dealing with a potentially dangerous drug.
None of us can imagine her state of mind but I do believe in that moment she thought it was the right drug. Being a control drug I am not sure if a re-entry would be enough- we get desensitized to alarms and alerts from constant exposure.
I know it is not the same thing, but I have has students who have intranasal Versed ordered for seizures in a school setting. It is not IV, but this story made me really think about it in a way I never did before. Sometimes when you are so familiar with a drug you just don’t think about the risk it carries.
And by monitoring- did they mean being on a monitor? Or monitored by someone? That part could be confusing- apparently she was not on a monitor or they would have caught this situation earlier. I suppose either would have helped it to be caught earlier.
The whole situation was fraught with risk. People do not realize how we hold life in our hands every day. Even truckers are not allowed to drive for more than 11 hours but we are supposed to endure for as long as it takes.
I love the analogy of the truck driver. Most things that we do, like truck drivers, do not pose an immediate risk to people. We’re not like a surgeon with a sharp instrument. That’s why errors like these are so scary. Any nurse, performing routine care has the ability to seriously harm or kill a patient. If we worked at Taco bell and gave the wrong order to the wrong customer at the wrong time, nobody is hurt. We choose to be nurses and that choice entails risk. Anyone who hasn’t spent time as a nurse is unfit to judge.
I love the idea of Intranasal Versed. Problem solved.
I understand what you mean about monitoring. In my head, I figured it was monitoring by a nurse but it could also mean cardiac and pulse ox monitors. Either or both might have prevented this.
Remember in nursing school where all procedures began with, “Wash hands. Provide for Adequate Lighting”. I understand now.